I would like to dedicate this project to many people that were beside me throughout this long exciting journey, without their unrelenting confidence and support I couldn’t have come so far.
To my father Fouad, thank you for teaching me how to live intelligently and how to be honest, just and fair, thank you for your patience and understanding, you are a real father, I will always remember your words and I will keep them locked in my heart; may your sole rest in peace.
To my mother Jeannette, thank you for your tenderness, devotion and sacrifice, you are the best mom in the world, I’m forever grateful to you; may god protect you.
To my sister Mireille and brother Toni, thank you for being here throughout this long journey, you have always been so supportive and encouraging.
To Frederika and Selim, thank you for supporting those who supported me.
To Karl, Romy and Kaline, you are my daily source of joy, I wish you a prosperous and joyful life.
Alfred F. Ammoury
To all soft bright smiles and faces that followed my hard long nights, to those hands that drove me to the road of success: to my parents.
I warrantly thank my parents for their assistance, great affection and help to realize my dreams.
Wissam f. Derian
How small and cheap words become when faced with unlimited love and endless sacrifice.
To mom, for her magnificent devotion to her family, for teaching me to accept pain with joy and hope, and to celebrate success with modesty and grace, for giving everything she had even with her ending breath.
To dad, for the uncompromising principles that guided his life, for leading his children into intellectual pursuits, for teaching me to treat patients as human beings not cases.
To Joelle, for filling the gap life has made, for being an example of optimism and hard working, for showing me the joy and excitement of studying medicine.
To Tony and Jessy, for their abundant support, for their patience and understanding and for their love.
For being just as they were.
Gino. S. Gemayel
Acknowledgments
This project is a tribute to the patients that we met throughout our internship. Each day we are reminded how truly precious are patients and what an honor it is to care for them.
We would like to thank a great many people that were instrumental in the creation of this project.
First, we owe a special thanks to Dr. Hadi Karaa, whose limitless understanding and support allows us to pursue projects such as this, without his invaluable advice and encouragement none of this would be possible.
We would also like to express our sincere and deep appreciation to Dr. Fouad Farhat, Dr. Joseph Haddad and Dr. Antoine Ferzly who gave liberally of their time to evaluate this project, without the extraordinary talent and commitment of these physicians we couldn’t have come so far.
A special thanks to our teachers who have been inspirational and instrumental in our education over the past 7 years especially Dr. Becharra Chahoud, Dr. Pierre Yared, Miss Dina Khairallah and Miss Lena Romanous.
![]() Finally
we like to thank Miss Leila Haouzy and Mrs. Wadiaa Jabr for the patience, help
and advice in the design and execution of this project----Could we add one more
thing please?
Finally
we like to thank Miss Leila Haouzy and Mrs. Wadiaa Jabr for the patience, help
and advice in the design and execution of this project----Could we add one more
thing please?
Alfred F. Ammoury
Gino S. Gemayel
Wissam F.Derian
Carcinoid tumors are endocrinologic malignancies often associated with a characteristic syndrome – the malignant carcinoid syndrome.
Cardiovascular manifestations of this rare illness result from unique pathophysiologic characteristics, are associated with poor prognosis, and are difficult to treat medically. The hemodynamic consequences of this disease present unique management problems perioperatively. New pharmacologic and surgical therapies for malignant carcinoids have improved quality of life for patients to extent that carcinoid heart disease now has more impact on morbidity and mortality rates. Cardiologists may be called on to diagnose and treat this rare cardiac disease. We review, for consulting cardiologists, the pathophysiologic characteristics, cardiovascular manifestations, and management of this disease.
Carcinoid tumors are the most frequently encountered endocrine tumors of the gastro intestinal tract, they comprise 55% of all gastrointestinal end endocrine tumors.
However, the overall incidence of this tumor is only 1.5 cases per 100.000 of the general population.
They are most often found in the appendix, although they can arise in any location of the gut.
Carcinoid tumors may secrete a variety of bioactive substances, which can cause the complex of symptoms associated with the carcinoid syndrome that develops in only 20% to 30% of patients with these tumors. Carcinoid heart disease, a rare form of valvular heart disease, develops in 50% to 60% of patients with carcinoid syndrome, which is distinguished classically by secretory diarrhea, cutaneous flushing, bronchoconstriction and hemodynamic instability in patients with malignant carcinoid tumors. Insights into the pathophysiologic characteristics of carcinoid disease have led to the development of novel medical and surgical therapies that improve symptoms and may prolong life.
Because the associated cardiac complications have become a major cause of illness and death, a thorough understanding of the pathophysiologic characteristics of this tumor and its cardiovascular effects necessary for the consulting cardiologist.
Although the gross pathology of carcinoid tumors was probably first described by Langhans in 1867, Lubarsch is credited with the original detailed description of these lesions in 1888. He reported the autopsy findings of a patient with multiple carcinoid tumors involving the ileum.
The classic symptomatology of the carcinoid syndrome was reported two years later by Ransom. He described a patient with diarrhea and wheezing secondary to an ileal carcinoid that had metastasized to the liver. The term karzinoid was introduced in 1907 by oberndorfer to describe these tumors because of their relatively benign behavior compared with gastrointestinal adenocarcinomas. The derivation of carcinoid tumors from argentaffin-staining enterochromaffin cells of the gastrointestinal (GI) tract was postulated by Gosset and Masson in 1914. The description of 5-hydroxytryptamine (serotonin [5-HT]) in 1948 was followed by a flurry of discoveries regarding the endocrine potential of carcinoid tumors. Carcinoid heart disease was just described in 1952 in a young man with pulmonic stenosis, tricuspid regurgitation, asthma, and “cyanosis” who died after cardiac catheterization and was found to have metastatic carcinoid disease.
In 1952, serotonin was identified as the primary secretory product of enterochromaffin cells of the gut, and in 1953, serotonin isolated from an ileal carcinoid tumor. The carcinoid syndrome, which consists of cutaneous flushing, bronchospasm, diarrhea, and right-sided valvular lesions, was then described by Pernow and Waldenstrom in 1954.
Finally, in 1955, Page and associates reported the secretion of large quantities of 5-hydroxyindoleacetic acid (5-HIAA), the metabolite of serotonin, in the urine of patients with carcinoid tumors.
PATHOLOGY AND CLASSIFICATION OF
CARCINOID DISEASE
Histologically, carcinoid tumors are composed of small epithelioid cells, with a low mitotic index and occasional acinar or rosette formation (Fig. 1A-B). However, slight histologic variation is not uncommon among carcinoids. Five histologic types of carcinoid tumors have been identified (Table I). Tumors that display a mixture of acinar and glandular features have the best prognosis with a median survival time approaching 4.5 years. Poorly differentiated tumors carry the worst prognosis (0.5 years).
Carcinoid tumors also may be grouped according to the embryologic site of origin. The classification system proposed by Williams and Sandler identifies the tumors as arising from the foregut, midgut, or hindgut. Although this may seem oversimplified and is considered archaic by some, tumors arising from each region have unique biologic characteristics and can cause different symptoms (Table 2 and 3). Foregut tumors arise in the lungs, stomach, or proximal duodenum and constitute approximately 15% to 25% of all carcinoids. They generally have a low serotonin content and may produce a variety of other bioactive agents, including 5-hydroxytryptophan (5-HTP), corticotropin, tachykinins, and gastrin. Midgut tumors are the most common variety of carcinoids. They may arise in the appendix (30% to 50% of all carcinoids), the small intestine (15% to 35% of all carcinoids), or the right colon. Midgut tumors commonly produce serotonin and tachykinins and are responsible for the carcinoid syndrome when metastases to the liver are present. Although appendiceal carcinoids occur far more frequently than carcinoids of the small intestine, they are usually neither invasive nor metastatic and do not cause the carcinoid syndrome. Tumors with high metastatic potential generally arise from either Midgut (distal duodenum, jejunum, ileum, and right colon) or foregut structures (bronchi, stomach, and proximal duodenum).
Hindgut Carcinoids occur less frequently and tend to follow a benign course they are found in the distal colon and rectum. While these lesions do not classically produce serotonin, substances including somatostatin and peptide YY have been immunolocalized to hindgut carcinoids
All carcinoid tumors produce a wide variety of physiologically active substances, including 5-hydroxytryptamine (serotonin), 5-hydroxytryptophan, histamine, bradykinins, tachykinins, and prostaglandins. The clinical syndrome in a given patient reflects the type of tumor and its secretory products as well as the balance of these hormonal influences on target tissues. The synthesis and action of serotonin and bradykinin, two of the most common products, are discussed below.
a. Serotonin (5-Hydroxytryptamine |5-HT|)
Serotonin, a metabolic derivative of the amino acid tryptophan, is involved in a wide range of physiologic processes, serving as a CNS neurotransmitter, a melatonin precursor, and a platelet aggregation promoter. Serotonin is formed in carcinoid cells after the uptake of tryptophan (Fig. 2), which then undergoes hydroxylation by tryptophan dehydrogenase to give 5-hydroxytryptophan (5-HTP), this is then rapidly converted to serotonin (5-HT) by decarboxylation by an enzyme called dopa decarboxylase.
Once secreted, serotonin is oxidized and dehydrogenated by monoamine oxidase and aldehyde dehydrogenase found in the liver, lungs, and blood stream to produce 5-hydroxyindoleacetic acid (5-HIAA), which is ultimately excreted by the kidney.
The classic biochemical identification of carcinoid tumors involves quantifying the excretion of 5-HIAA in a 24-hour urine sample. Normal values for this assay range between 2 to 8mg per 24-hour period. Patients with a normal 24-hour excretion of 5-HIAA may undergo provocative testing with pentagastrin if a high clinical suspicion for carcinoid tumor exists.
Serotonin produced by carcinoid tumors in the gut is secreted into the portal circulation and metabolized within the liver. As a result of this first-pass effect, most carcinoid tumors do not cause the features of carcinoid syndrome until after hepatic metastases develop and these hormones can be secreted directly into the systemic circulation. Similarly, the presence of these degrading enzymes in pulmonary endothelial cells may also explain why left-sided cardiac involvement is uncommon in this syndrome except in cases of right-to-left shunting, bronchial tumors, or pulmonary metastases.
Approximately 90% of the body’s serotonin is normally produced and stored within the cells of the gut; 10% is found in platelets, and a small amount is found within the central nervous system. In humans, most tryptophan is used in the synthesis of protein and niacin – only 1% is metabolized to serotonin.
However, in patients with carcinoid tumors up to 60% of tryptophan is used in serotonin synthesis. As a result niacin deficiency and pellagra can develop.
Serotonin acts on smooth muscle receptors to increase intestinal motility and produce bronchial constriction and uterine contraction. Vasoconstriction is induced directly by activation of specific cell surface receptors (5-HT1 and 5-HT4) and indirectly by potentiating the actions of histamines, norepinephrine, and angiotensin II.
Paradoxically, serotonin can also cause vasodilatation by binding to a different subtype of 5-HT1 receptors. Positive chronotropic and inotropic effects, also mediated by 5-HT1 receptors on cardiac muscle, have also been observed. Serotonin has been shown to stimulate fibroblasts. Table 4 depicts the complex effects of serotonin.
b. Bradykinins:
Carcinoid tumors also produce kallikreinins that enzymatically convert kininogen to bradykinin. Peripheral effects of bradykinin include hypotension, vasodilatation, increase capillary permeability, bronchoconstriction, and increases in nonvascular smooth muscle tone. Tachykinins such as substance P, neurokinin A, and neuropeptide K are also elevated in a subset of patients with carcinoids; substance P may be involved in the development of the carcinoid flush.
Clinically, this syndrome develops when the vasoactive substances produced by a carcinoid tumor escape hepatic degradation and gain access into the systemic circulation.
The classic carcinoid syndrome of cutaneous flushing, secretory diarrhea, and valvular heart disease is present in 25% of patients with carcinoid tumors and is most common in patients with small bowel tumors and hepatic metastases. In rare instances when these symptoms are present without hepatic metastases, the primary tumor is usually localized to the bronchus or ovary and secretes hormones directly into the systemic circulation (Fig. 2).
Less frequent examples include carcinoid tumors with extensive retroperitoneal involvement that drain into the paravertebral venous system. Other symptoms and signs associated with the carcinoid syndrome include wheezing and telangiectasias. Paroxysmal hypotension, often accompanied by cutaneous flushing, describes the classic “carcinoid crisis”. Interestingly, symptoms vary somewhat with the type and location of the primary tumor. All carcinoid tumors produce tryptophan dehydroxylase and dopa decarboxylase, but in different concentrations. This enzymatic variation accounts for some of the diversity of hormone production by these tumors. For example, foregut tumors are rare, and patients who have them tend to have prolonged flushing. These tumor cells contain lower levels of dopa decarboxylase resulting in the higher levels of 5-hydroxytryptophan.
In contrast, hindgut tumors tend to produce lower levels of 5-hydroxytryptophan and 5-hydroxyindoleacetic acid, and symptoms are rare. Furthermore, gastric carcinoids tend to secrete larger amounts of histamine, and bronchospasm is a more prominent clinical finding. Two types of cutaneous flushing have been described. Patients with the carcinoid syndrome secondary to midgut tumors demonstrate faint pink to red flushing that begins in the face and spreads to the trunk or extremities. Patient with foregut carcinoids demonstrate a much darker, purplish flushing that involves the upper trunk and limbs. Flushing can be precipitated by stress or by consuming blue cheese, chocolate, alcohol, and wine. Diarrhea is present in approximately 75% of patients with the carcinoid syndrome and is typically exacerbated by episodes of cutaneous flushing.
Bronchoconstriction and dyspnea associated with a flushing episode also have been reported in 25% to 30% of patients. Right-sided cardiac valvular disease can occur in up to one third of patients. Patients develop pulmonic and tricuspid fibrosis, which ultimately leads to valvular incompetence. If the primary carcinoid is slow growing, patients with carcinoid-syndrome-associated valvular disease are candidates for valve replacement. Cardiac failure in this setting implies a poor prognosis. Serotonin is believed to be largely responsible for the diarrhea, fibrosis, and cardiac valvular disease seen in patients with the carcinoid syndrome. However, the exact substances responsible for the vasomotor changes are unknown.
Patients with the carcinoid syndrome excrete elevated levels of 5-HIAA during a 24-hour urine collection. Whole blood or platelet-poor plasma serotonin levels are also elevated in most patients. A useful test in equivocal situations is the pentagastrin provocative test, which induces flushing, gastrointestinal symptoms, and an elevation in circulating serotonin levels. Enhanced releases of other neuroactive substances (eg, substance P, neuropeptide K, and neurokinin A) also may occur.
The median survival for patients with carcinoid syndrome is 38 months. Long-term survival and quality of life depend largely on the control of tumor growth and suppression of the amine-induced symptoms.
In approximately 20% of patients with carcinoid disease, the presenting symptom may be attributable to heart failure. The cardiovascular effects of carcinoid disease include structural damage to the heart and hemodynamic derangements – both are related to the effects of tumor secretions. Although direct myocardial metastases are occasionally seen, structural damage is generally from the cardiac plaque.
Carcinoid heart lesions are characterized by plaquelike, fibrous endocardial thickening that classically involves the right side of the heart and often causes retraction and fixation of the leaflets of the tricuspid and pulmonary valves (Fig. 3).
Although carcinoid disease is sometimes inaccurately perceived as an infiltrative process, the carcinoid plaque is actually superficial, adherent to the surface of the endocardium and limited by endocardial elastic fibers. This plaque, regardless of its location within the heart, is composed of smooth muscle cells, myofibroblasts, and an overlying endothelial cell layer. Smooth muscle cells and myofibroblasts are surrounded by an extracellular matrix composed of microfibrils, acid mucopolysaccharides, basement membrane, and collagen fibers. Interestingly, elastic fibers, abundant in myocardial tissue, are not seen in these plaques. The exact pathogenesis of these plaques is unknown; however, animal studies have demonstrated that serotonin infusion in the presence of hepatic injury or tryptophan or niacin deficiency may induce the formation of lesions similar to the human cardiac plaque. Bradykinin has also been implicated because it can cause endothelial damage and is inactivated in the pulmonary circulation, thus limiting left heart exposure. Given the frequent location of these plaques on the endothelial side of valves, turbulent blood flow may also contribute to plaque localization.
Cardiac involvement is seen in up to 60% of patients with metastatic carcinoid. Right heart disease is severe in 25% of patients with cardiac involvement. The severity of cardiac damage appears to be proportional to the urine levels of 5-HIAA levels.
Cardiac disease is rare in gastric carcinoids, where 5-hydroxytryptophan and histamine are the predominant secretory products. Left-sided cardiac involvement is rarely seen except in patients with bronchial carcinoids or right-to-left intracardiac shunts. In these instances the left heart disease is usually less severe and involves the mitral valve. Mild to moderate mitral regurgitation is usually the only result. In addition to the cardiac valves and endocardium, plaque deposition has also been demonstrated in the vena cavae, pulmonary artery, coronary sinus, and coronary arteries. Valvular disease is the most common cardiac pathologic feature, and the tricuspid valve is most commonly affected. Tricuspid damage was observed in 97% of patients in the largest reported series of 75 patients. The pulmonic valve was involved in 88% of the cases, with 49% of patients displaying significant pulmonic stenosis and 81% pulmonic insufficiency. Patients were typically seen with signs suggesting right heart failure from tricuspid stenosis and regurgitation and pulmonic stenosis. Left-sided cardiac involvement was seen in only 7% of patients. Five of these patients in the series had bronchial carcinoids, three had patent foramen ovales, and one patient had four-valve involvement with no evidence of intracardiac shunt or pulmonary involvement. All patients with left heart involvement were also noted to have right heart involvement. Intracardiac metastases were seen in 4% of patients, all of whom had ileal tumors. Small pericardial effusions of no hemodynamic significance were seen in 14% of cases.
The hemodynamic effects of carcinoid secretions can range from the marked hypotension of carcinoid crisis to severe hypertension refractory to intravenous vasodilators. These extremes of vasomotor tone represent the interplay between the principle hormone secreted, the relative concentrations of the various tumor hormones, the predominant receptor effect, and resting vascular tone. In patients with increased baseline vascular tone, serotonin may produce hypotension whereas in those with reduced baseline tone serotonin may increase peripheral resistance. Bradykinin is believed to precipitate the triad of the classic carcinoid crisis: hypotension, bronchospasm, and cutaneous flushing. Serotonin induces hypertension, tachycardia, and transient hyperglycemia.
The implications for cardiac involvement are profound, as patients without cardiac involvement in one series had a 68% 3-year survival, whereas those with cardiac lesions had only a 31% survival over the same interval. Mean life expectancy was 1.6 years for patients with carcinoid heart disease versus 4.6 years in those without cardiac damage. Treatment of the underlying cardiac manifestations may decrease mortality rate and palliate refractory symptoms. Cure is only rarely achieved in patients with carcinoid tumors, specifically those with limited non metastatic disease. However, tumor progression is very slow and patients may survive for years. Thus both medical and surgical therapy for symptom palliation is an important consideration.
Dexfenfluramine was approved in the United States for long-term use as an appetite suppressant until it was reported to be associated with valvular heart disease. The valvular changes (myofibroblast proliferation) are histopathologically indistinguishable from those observed in carcinoid disease or after long-term exposure to 5-hydroxytryptamine (5-HT)(2)- preferring ergot drugs (ergotamine, methysergide). 5-HT(2) receptor stimulation is known to cause fibroblast mitogenesis, which could contribute to this lesion. To elucidate the mechanism of “fen-phen” – associated valvular lesions, we examined the interaction of fenfluramine and its metabolite norfenfluramine with 5-HT (2) receptor subtypes and examined the expression of these receptors in human and porcine heart valves.
Fenfluramine binds weakly to 5-HT (2A), 5-HT (2B), and 5-HT (2C) receptors. In contrast, norfenfluramine exhibited high affinity for 5-HT (2B), and 5-HT (2C) receptors and more moderate affinity for 4-HT(2A) receptors. In cells expressing recombinant 5-HT(2B) receptors, norfenfluramine potently stimulated the hydrolysis of inositol phosphates, increased intracellular Ca (2+), and activated the mitogen-activated protein kinase cascade, the latter of which has been linked to mitogenic actions of the 5-HT (2B) receptor. The level of 5-HT (2B) and 5-HT (2A) receptor transcripts in heart valves was at least 300-fold higher than the levels of 5-HT (2C) receptor transcript, which were barely detectable. We propose that preferential stimulation of valvular 5-HT (2B) receptors by norfenfluramine, ergot drugs, or 5-HT released from carcinoid tumors (with or without accompanying 5-HT (2A) receptor activation) may contribute to valvular fibroplasia in humans.
The presentation of a carcinoid tumor varies according to its site of origin. The most common occurring sites of foregut carcinoids are the bronchus and stomach. Bronchial carcinoids are usually slow-growing tumors that arise in the proximal bronchus and primarily produce symptoms of bronchial obstruction and hemoptysis. Carcinoids arising in the stomach are generally incidentally identified unless they produce upper abdominal pain, bleeding, or obstruction of the gastric outlet. Midgut tumors occurring in the appendix and small bowel are frequently silent and therefore may be locally advanced when discovered. The presentation of appendiceal carcinoids may be indistinguishable from that of acute appendicitis. Tumors of the small intestine generally grow slowly and produce symptoms of intermittent abdominal pain and weight loss. Malignant carcinoids in this region induce significant fibrosis in the small bowel mesentery and are associated with mechanical small bowel obstruction. Rectal carcinoids can cause rectal bleeding and are frequently noted on rectal examination or lower endoscopy. When a carcinoid tumor is suspected, the appropriate workup should include a careful functional and anatomic characterization of the tumor.
In the case of cardiac involvement the main clinical signs are dyspnea and asthenia rendered ingravescent by effort, and, in the latter stage, a frank picture of congestive cardiac decompensation.
On Auscultation, stethoscopic evidence of tricuspid valvulopathy, combined or not with pulmonary valvulopathy is present. The ECG picture may display a constant reduction in cardiac potentials, together with right branch bundle block.
Several techniques are available to evaluate the primary location and extent of disease for carcinoid tumors. Patients with signs and symptoms suggestive of a bronchial carcinoid should undergo bronchoscopy and computed tomography (CT) scan of the chest. On bronchoscopy, foregut carcinoid appear as deep pink or red tumors that protrude into the bronchial lumen. A CT scan of the chest is useful to determine regional lymph node involvement, which occurs in approximately 10% of patients. Carcinoid tumors of the stomach are usually identified with upper endoscopy or upper GI series during the evaluation of peptic ulcer symptoms or upper GI bleeding. CT scans of the abdomen and pelvis are helpful in evaluating tumor spread to the liver and/or regional lymph nodes. Upper and lower endoscopy, enteroclysis, upper and lower GI series, and CT scans of the abdomen and pelvis are important tools in the workup of midgut and hindgut carcinoid tumors. Midgut tumors are most frequently associated with tumor extension into the mesentery and distant spread to the liver. They frequently cause retroperitoneal fibrosis and ureteric obstruction. These findings are easily demonstrated by CT scan. Mesenteric angiography may show caliber changes or outright occlusion of blood vessels suggesting tumor encasement of the superior mesenteric artery or its branches. Finally, when attempts at anatomic localization have been unsuccessful but the presence of a carcinoid tumor is fairly certain based on biochemical studies, exploratory laparotomy may provide both diagnostic and therapeutic benefit.
The diagnosis of carcinoid tumors is based on the combination of suggestive pathologic features and elevated urine 5-HIAA. Carcinoid tumor cells are small, round, monotonous lymphocytic-appearing cells (Fig. 4). They are usually argyrophilic or argentaffin staining and may also stain with a variety of immunohistochemical labels. 5-HIAA Levels normally range from 0 to 8mg/ 24hours. Slight elevations may be seen in patients consuming a diet rich in tryptophan (nuts, bananas, pineapple, kiwi, and avocados) and taking the drugs guaifenesin or acetaminophen; conversely, aspirin and levodopa may falsely lower levels. In the setting of carcinoid disease, levels typically range from twice normal to as much as 800 to 1000 mg/day. In some instances, when tumors are relatively deficient in dopa decarboxylase, serum levels of 5-hydroxytryptophan may be useful in making the diagnosis. Injection of radiolabeled metaiodobenzylguanidine (MIBG) or octreotide, which has an affinity for the malignant cells, followed by isotope scanning may be performed to localize areas of uptake that suggest tumor.
The diagnosis of carcinoid heart disease is best made by echocardiography. The cardiac manifestations may be easily demonstrated with a combination of two-dimensional and Doppler techniques. Tricuspid valve involvement presents as a combination of stenosis and regurgitation from restricted leaflet mobility from plaque deposition on the leaflets (Fig. 5 and 6). The Doppler pattern of increased tricuspid inflow velocity suggests stenosis (although it is also consistent with increased flow across the valve from tricuspid regurgitation), whereas a dagger-shaped regurgitation velocity signal indicates rapid equilibration of right atrial and right ventricular systolic pressures from severe valvular incompetence. It should be noted that the severity of pulmonic stenosis may be underestimated because of low cardiac output and severe tricuspid regurgitation.
d. Echocardiographic Spectrum
Between 1980 and 1989, 132 patients with carcinoid syndrome underwent echocardiographic study. The echocardiographic, Doppler, and clinical features of the 74 patients (56%) with echocardiographic evidence of carcinoid heart disease are described. Among these patients, 97% had shortened, thickened tricuspid leaflets. Tricuspid regurgitation was present in all 69 patients with carcinoid heart disease who underwent Doppler examination, and it was of moderate or severe degree in 62 patients (90%). Severe tricuspid regurgitation was characterized by a dagger-shaped Doppler spectral profile with an early peak pressure and rapid decline. The pressure half-time was prolonged (mean, 116 msec), which is consistent with associated tricuspid stenosis. The pulmonary valve appeared thickened, retracted, and immobile in 36 patients (49%) and was diminutive to the extent of not being visualized in an additional 29 patients (39%). Among the 47 patients who underwent Doppler evaluation of the pulmonary valve, regurgitation was present in 81%, and stenosis was present in 53%.
Left-sided valvular involvement was present in five patients (7%), four of whom had patent foramen ovale or carcinoid tumor involving the lung. Previously undescribed myocardial metastases were present in three patients (4%) and were confirmed by biopsy in each case. Small pericardial effusions were present in 10 patients (14%). Patients with and without echocardiographic evidence of carcinoid heart disease did not differ with regard to sex, age, location of the primary tumor, duration of diagnosis, or duration of symptoms of carcinoid syndrome. However, the mean pretreatment level of urinary 5-hydroxyindoleacetic acid was higher in patients with carcinoid heart disease than in patients without carcinoid heart disease (270 versus 131 mg/24hrs, p < 0.001). The symptom of dyspnea was more prevalent among patients with carcinoid heart disease than in patients without the disease (54% versus 27%, p = 0.003); as expected, heart murmur were also noted more frequently in patients with disease (92% versus 43%, p < 0.0001). Treatment regiments and response to therapy were similar in the two groups. Survival of patients with echocardiographic evidence of carcinoid heart disease was reduced compared with those without cardiac involvement (p = 0.0003). ECG and chest roentgenographic findings in patients with carcinoid heart disease were nonspecific.
CORRELATION OF HIGH SEROTONIN LEVELS WITH VALVULAR ABNORMALITIES DETECTED BY CARDIAC CATHETERIZATION AND ECHOCARDIOGRAPHY
Although serotonin has been indirectly linked to carcinoid heart disease, no direct evidence for different ambient serotonin levels in carcinoid cardiac and non cardiac patients has previously been reported. We will demonstrates that carcinoid patients with heart disease exhibit higher circulating serotonin levels than do their counterparts without heart disease. This finding supports the contention that serotonin plays a role in the pathogenesis of carcinoid heart disease.
In selected 604 carcinoid patients nineteen patients with proven carcinoid heart disease (by cardiac catheterization and/or echocardiogram) were compared with the remaining 585 non cardiac patients in the database with regard to circulating serotonin and its principal metabolite, 5-hydroxyindole acetic acid (5-HIAA).
No significant differences between the cardiac (n=19) and non cardiac groups (n=585) were seen with respect to race, sex, age at onset of carcinoid tumor symptoms, and age at diagnosis of carcinoid tumor (Table 5). Symptoms of flushing and diarrhea were almost threefold more common in the cardiac group (Table 5). Fig 7 shows the locations of primary carcinoid tumors. Although the non cardiac group had a wide distribution of primary tumor sites, the cardiac group exhibited a heavy preponderance of small intestine tumors (47%) and tumors of unknown primary location (48%).
The principal finding is that circulating serotonin levels were more than twofold higher in the cardiac group compared with the non cardiac group. (Fig 8). Specifically, cardiac patients demonstrated higher (P < .0001) levels of serum serotonin (9750 ± 4130 versus 4350 ± 6460 pmol/ml), plasma serotonin (1130 ± 1210 versus 426 ± 1130pmol/mL), and platelet serotonin (6240 ±4030 versus 2700 ± 2880 pmol/mg protein). Urine levels of the serotonin metabolite 5-HIAA were almost fourfold higher (P<.0001) in the heart disease patients compared with the non cardiac group (219 ± 124 versus 55.3 ± 141 mg/24 h).
Elevated serum serotonin (above the upper limit of normal range, i.e., > 1500 pmol/ml) was 100% sensitive but only 46% specific for carcinoid heart disease. Furthermore, there was no clear cutoff point in serotonin level that delineated the two groups.
Elevated urinary 5-HIAA is a less-than-ideal serotonin surrogate because it misses 10% of patients with true elevated circulating serotonin levels. These patients can be identified by direct measurement of circulating serotonin in the blood or plasma; however, because the majority of circulating serotonin is taken up and carried in the dense granules of platelets, platelet serotonin level is perhaps the most useful measure of the circulating hormone. The present study includes three different measurements of circulating serotonin (serum, plasma, and platelets); it is the first to directly demonstrate elevations of circulating serotonin in cardiac patients relative to patients without heart disease. Indeed, the twofold to fourfold higher levels of serotonin and 5-HIAA in the cardiac group may be an underestimation of the difference. Our stringent definition of heart disease may have resulted in the inclusion of some undocumented heart disease patients in the “non cardiac” group, a misclassification that would be expected to bias toward the null hypothesis.
Although this novel finding is consistent with a causal role for serotonin in the pathogenesis of heart disease, it is not proof. The high sensitivity (100 %) and low specificity (46%) of elevated serum serotonin level as a marker for heart disease suggest that elevated circulating serotonin is a necessary but not a sufficient component in the development of heart disease. Some other factor (eg, duration of high levels, cofactor, or genetic predisposition) may play a role in determining who will get heart disease. It is possible, for example, that the same tumors that secrete high quantities of serotonin also secrete high quantities of other agents that are causative or synergistic with serotonin in producing the characteristic fibrotic damage of the heart. Such a scenario would explain the absence of heart disease in some carcinoid patients with high circulating serotonin.
Of the 16 cardiac patients who had echocardiograms performed, 13 (81%) had evidence of right atrial and right ventricular enlargement by echocardiogram; 9 (56%) had evidence of a thickened or immobile tricuspid valve. Table 6 details the valvular abnormalities in this subgroup. The results for the 13 patients who underwent cardiac catheterization are similar and also are shown in Table 6. Tricuspid valve disease (especially regurgitation) was most prevalent. Left-sided valve lesions tended to be less common and of milder severity than their right-sided counterparts. Cardiac catheterization and echocardiography had an overall concordance of 91% on the basis of valvular lesions assessed by both methods.
Further review of the subgroup of cardiac patients who underwent catheterization showed that 12 (92%) had New York Heart Association class III or IV symptoms of congestive heart failure, and 1 (8%) had class II symptoms. Table 7 gives the hemodynamic profile of the group. Right-sided filling pressures tended to be mildly to moderately elevated (mean right atrial pressure > 10 mm Hg in 8 patents and > 20 mm Hg in 3 of these), whereas left-sided filling pressures were generally normal (mean pulmonary capillary wedge pressure >10 mm Hg in 3 patients and >20 mm Hg in 0 patients). This is consistent with the greater prevalence and severity of tricuspid and pulmonic valve diseases compared with mitral and aortic valve diseases.
Significant coronary artery disease (defined as at least 75% diameter stenosis in at least one major coronary artery or first-order branch) was noted in 5 of the 13 patients who underwent catheterization: 3 had single-vessel disease, 1 had two-vessel disease, and 1 had three-vessel disease.
Although coronary fibrosis has been propounded as a potential mechanism of coronary insufficiency in carcinoid patients, it is more likely that our finding is due to superimposition of a common disease (coronary atherosclerosis) on an uncommon one (carcinoid heart disease). Consistent with this is the observation that, at the time of catheterization, the mean age of the cardiac patients was 62.4 years; indeed, 4 of the 5 coronary artery disease patients were over the age of 65. Western epidemiological studies suggest an overall prevalence of coronary artery disease of about 25% in the elderly.
The survival was measured from each of two different starting points: from the onset of the first carcinoid tumor symptom (i.e., symptom of local tumor growth, metastatic disease, or carcinoid syndrome) and from diagnosis of carcinoid tumor. Regardless of which starting point was used, survival between the cardiac and non-cardiac groups was statistically different (Table 8). Furthermore, there was not even a clear trend because survival from onset of symptoms and survival from diagnosis of carcinoid tumor showed disparate trends.
In general, survival rates for carcinoid tumors are directly related to both the size of the primary tumor and evidence of distant metastatic disease. Resectional therapy for bronchial carcinoid had yielded a five-year survival rate of approximately 90% to 95%. Features associated with a poor prognosis include tumors larger than 3cm in size, positive lymph nodes, and atypical histologic features.
The reported five-year survival rate for patients with “sporadic” gastric carcinoid tumors is 52% for tumors of all stages. Patients with local lesions have a 93% five-year survival rate. Patients with regional lymph node or distant metastases have a poorer prognosis, with approximately 25% and 0%, respectively, surviving more than five years. Gastric carcinoid tumors associated with a hypergastrinemic state carry a favorable prognosis with a reported five-year survival rate ranging between 80% and 100%. The prognosis for patients with carcinoid tumors of the appendix is the most favorable of all the midgut carcinoid tumors. Tumors smaller than 2 cm in size that are treated with simple appendectomy carry five-year survival rates of 90% to 100%.
Of all the carcinoid tumors, small bowel carcinoid tumors are most likely to be associated with regional lymph node disease or hepatic metastases. With resectable nodal disease, median survival is 15 years, but this decreases to five year with nonresectable abdominal tumors and to three years with liver metastases at the time of presentation. Small bowel carcinoids less than 2 cm in size that are not associated with distant spread carry a prognosis that is no different from that of the general population. Rectal carcinoids also carry a favorable prognosis, with tumors less than 2 cm in size having a five-year survival rate approaching 100%.
a. Medical therapy:
Medical therapy for carcinoid disease with or without cardiac involvement consists of cytotoxic chemotherapy, long-term drug therapy for symptomatic relief, and medications for perioperative management (Table 9).
Medical management of the carcinoid syndrome has focused on cytoreductive chemotherapy and pharmacologic control of the bioactive substances produced by these tumors. Response rates approaching 40% have been reported for combined chemotherapy with streptozotocin and doxorubicin in small groups of patients. However, the responses have been short-term and the chemotherapy regimen carries significant side effects. Octreotide, a somatostatin analog, is the most effective pharmacologic agent available to ameliorate the symptoms associated with the carcinoid syndrome. Octreotide has been shown to inhibit the synthesis and release of bioactive substances by carcinoid tumors. The significant action of octreotide to enhance fluid absorption in the GI tract helps to diminish the secretory diarrhea of the carcinoid syndrome. Octreotide may be subcutaneously administered twice daily at an initial dose of 100 to 200 μg. The drug can then be titrated to effect, with more than 80% of patients showing symptomatic improvement at doses ranging between 500 and 1000 μg per day. Octreotide is also indicated for the prevention of a carcinoid crisis. Carcinoid tumors significantly increase the rate of bioactive peptide production when manipulated intraoperatively or when patient are stressed by anesthesia or chemotherapy. Pretreatment with octreotide will prevent these reactions.
The current recommendations are for the subcutaneous administration of 125 to 250 μg of octreotide every eight hours beginning 24 to 48 hours before the induction of anesthesia. Patients undergoing chemotherapy should receive a subcutaneous dose of 250 to 500 μg of octreotide approximately one to two hours before chemotherapy begins. Diaco et al have recently reported the use of hepatic artery chemoembolization in combination with hepatic artery 5-fluorouracil infusion and long-term octreotide therapy in 10 patients with the carcinoid syndrome. They found this regimen to be more effective than tumor embolization alone, systemic chemotherapy alone, or long-term octreotide therapy alone for control of tumor growth and carcinoid symptoms. This regimen also appears to provide an increased life expectancy and improve the quality of life for patients with carcinoid tumors metastatic to the liver. The regimen was well tolerated with few associated complications. A randomized, prospective, double blind trail seems warranted.
Somatostatin, a counterregulatory hormone, binds to cell surface receptors on carcinoid tumor cells (as well as normal cells) and inhibits the release of serotonin. With a plasma half-life of only minutes, it must be administered by continuous intravenous infusion. However, octreotide, a synthetic congener with a longer half-life, was developed and is now commonly used to manage the symptoms of carcinoid disease. Its use was first reported as a case series in 1986, and it was approved by the Food and Drug Administration in 1988 for management of chronic symptoms. Eighty-seven percent of the first 66 patients treated responded with reduced flushing, and 77% had less diarrhea. Seventy-seven percent also had a >50% reduction in 5-HIAA levels. There are also date from case reports and from a series of eight patients that pretreatment with octreotide can terminate perioperative hypotensive carcinoid crises and block the classic carcinoid crisis provoked by pentagastrin. Octreotide is now used routinely for both long-term symptomatic treatment and as preoperative prophylaxis to prevent hypotensive crises.
Historically, nonspecific serotonin receptor antagonists were used with mixed results to counteract the presumed effects of serotonin. These drugs included methysergide and cyproheptadine (also a histamine-1 receptor blocker).
The use of the selective serotonin receptor antagonist ketanserin (which also has some a 1-receptor-blocking effects) for the intraoperative management of severe hypertension refractory to vasodilators during cardiac valve replacement surgery has been described in case reports and a small series. Its use before the procedure to prevent hypertensive crisis has also been described in a case report. Ketanserin has Vaughn-Williams class I and III antiarrhythmic effects and has been reported to prolong the corrected QT interval. The risk of torsades de pointes may be increased in the setting of hypokalemia and hypomagnesemia. Case reports of its limited use in patients with carcinoids have noted no arrhythmic complications. It is not approved by the Food and Drug Administration for use in the United States.
Theophylline and steroids have been advocated for patients with bronchoconstriction; both selective and nonselective histamine receptor antagonists have been used for alleviation of the other effects of histamine, such as flushing and urticaria seen with gastric carcinoids. Although the use of these medications is intuitive and probably of minimal risk (except perhaps in the case of theophylline), objective data about the use of these agents are limited. Although there is some debate about their efficacy, most case reports describe the use of antihistamines both for chronic symptomatic treatment and for perioperative prophylaxis. Glucocorticoids are often administered perioperatively. Similarly, digoxin and diuretics, despite limited efficacy, are the main medical therapies for right heart failure in patients with carcinoid heart disease.
b. Surgical treatment:
Surgical treatment for carcinoid disease has included resection of the primary tumor for cure or debulking in the case of metastatic disease, resection of hepatic metastases, and cardiac valve surgery. Cure has only been achieved when non metastatic tumor has been completely resected. Patients with intractable right heart failure from carcinoid disease and well-controlled systemic symptoms have been considered for cardiac valve replacement.
Surgery is the primary treatment for bronchial carcinoid tumors. If possible, conservative procedures including sleeve resections or local bronchial resections with bronchoplasty should be undertaken. This conservative approach is advocated secondary to the relatively low malignant potential of bronchial carcinoids. Lobectomy is an acceptable alternative if these conservative procedures cannot be undertaken safely.
The management of gastric carcinoid had recently been reviewed by Gilligan et al. The hypergastrinemia found in association with chronic atrophic gastritis, Zollinger-Ellison syndrome with multiple endocrine neoplasia type1, and pernicious anemia is associated with an increased incidence of gastric carcinoid tumor formation. Tumors that develop in the setting of hypergastrinemia can be managed by endoscopic excision if they are less than 1 cm in size or fewer than three to five in number. Hypergastrinemic patients with carcinoid tumors that are larger than 1cm in size or more than three to five in number should undergo a distal gastric resection to remove the source of gastrin, as well as local excision of any proximal fundic lesions noted during surgery. Patients who undergo endoscopic polypectomy or distal gastric resection must be followed at six-month intervals with endoscopic surveillance and biopsy. Recurrences should be treated with surgical resection. The conservative management of gastric carcinoids in the setting of hypergastrinemia is related to their relatively low malignant potential.
Patients with “sporadic” gastric carcinoid tumors should be treated more aggressively. Generally, these are single tumors that arise against a background of normal gastric mucosa. “Sporadic” tumors usually are larger than 1cm in size and are not associated with an elevated plasma gastrin level. The metastatic potential of these lesions warrants a total gastrectomy and regional lymphadenectomy. Patients with metastatic disease to the liver may undergo concurrent hepatic resection if anatomically feasible.
The management of uncomplicated midgut carcinoid tumors is straightforward. Tumors that occur in the small bowel and right colon should be resected en bloc with their regional mesenteric lymph nodes. Tumors of the appendix less than 1 cm in diameter are unlikely to be metastatic and may be managed with simple appendectomy. Appendiceal carcinoids greater than 2cm in size demonstrate an increased incidence of regional spread and should be managed with a formal right hemicolectomy. Metastases from appendiceal carcinoids 1 to 2cm in size are rare, suggesting that lesions in this size range also may be safely managed with simple appendectomy. Appendiceal carcinoid tumors less than 2 cm in size that have positive lymph nodes at the time of surgery should be managed with a formal right hemicolectomy.
Midgut carcinoids can cause mechanical small bowel obstruction due to either direct tumor involvement or fibrosis of the surrounding mesentery. These large lesions constitute a significant threat to the well being of the patient and should be resected if technically feasible. These patients often have a foreshortened fibrotic mesentery, making dissection of vascular structures difficult. An error in mesenteric dissection may devascularize a significant portion of small bowel.
Carcinoid tumors involving the rectum also are managed in large part according to size. Lesions that are less than 1 cm in size may be managed by endoscopic or transanal excision. Tumors greater than 2 cm in size should be managed by low anterior resection or abdominoperineal resection. Locally excised tumors that demonstrate invasion through the muscularis propria should be managed by wider excision or anatomical resection.
Surgical cure for patients with the carcinoid syndrome is unusual, because many of these patients have significant metastatic deposits in the liver. Although few patients are amenable to complete resection of their hepatic metastases, anecdotal experience suggests that debulking hepatic metastases may palliate systemic symptoms. However, palliation is often brief and frequently associated with substantial morbidity.
Hepatic artery embolization is another alternative with results similar to those seen with hepatic resection, but this approach avoids the morbidity associated with a major operation. Ischemic treatment of hepatic metastases is successful principally because these lesions derive their blood supply form the hepatic artery. The remaining hepatic parenchyma receives adequate perfusion via the portal vein. There are several reports of successful palliation of the carcinoid syndrome by selective hepatic artery embolization. Side effects of this therapy include abdominal pain, fever, transient nausea, and emesis. Despite providing significant symptomatic improvement, hepatic artery embolization of hepatic carcinoid metastases may not result in a significant long-term survival benefit.
Hepatic transplantation also has been attempted in selected patients with promising results. Long-term follow-up is lacking, which precludes generalization of this treatment modality to the general patient population.
In one series of 26 carcinoid patients who underwent cardiac surgery, 25 of 26 had hepatic metastases and one patient had ovarian carcinoid. Tricuspid valve replacement was performed in all patients. Twenty-one of 26 patients had pulmonic valve gradients measured, and all were > 10mm Hg. Twenty-four of 26 underwent either pulmonary valvectomy with pulmonary annulus enlargement or pulmonary valve replacement (if left heart pressures were elevated) for the relief of right ventricular outflow tract obstruction. Both mechanical and bioprosthetic valves were used. Thirty-day mortality rate was 35% with deaths arising from bleeding complications and, in one instance in which pulmonic stenosis was not remedied, intractable right heart failure. After the first 6 months surgical patients tended toward increased survival when compared with medically managed patients, although the difference did not meet statistical significance. The 2-year survival was 40% in the surgically treated group versus 8% in the medically treated group. No medically treated patients were alive at 3 years. The only preoperative finding that correlated with poor operative prognosis was low voltage on the electrocardiogram. Increased bleeding complications were noted in patients older than 64 years and in those who had pleural or pericardial plaques. Late survival, as defined by those patients alive at the mean follow-up of 28 months, was predicted by lower somatostatin requirements and lower preoperative 5-HIAA levels. Six long-term survivors required 525 +/- 444mg octreotide/day versus 17 nonsurvivors who required 1142 + / - 648 mg/day (p=0.04). 5-HIAA Levels in the eight survivors were 133 +/- 97 mg/24 hours versus 210 +/- 97 mg/24 hours in the 18 nonsurvivors (p=0.04). No late death, from cardiac problems were recorded, but in two patients the cause of death was unknown.
All patients with newly diagnosed metastatic carcinoid disease as well as bronchial or ovarian carcinoids should undergo a complete echocardiographic examination to define the extent of cardiac involvement. Mild to moderate symptoms of chronic heart failure should be treated with diuretics and perhaps digoxin. Once right heart failure becomes refractory to medical management, valve surgery may be considered in selected patients. Bioprosthetic valves are now favored because long-term anticoagulation is generally not required, perhaps reducing the incidence of long-term bleeding complications in patients at risk for hepatic dysfunction. Also, initial concerns regarding damage to these valves from carcinoid have not been realized. Because the 5-year surgical survival of patients in the recent series was approximately 20%, long-term durability of bioprosthetic valves is not likely to be a major concern. Evaluation of pulmonic stenosis is of critical importance to minimize the risk of fatal postoperative right ventricular failure. A Doppler gradient > 10 mm Hg is considered by one group to be an indication for pulmonic valve replacement or removal.
For the cardiology consultant there are several considerations for the patient planned for cytoreductive or cardiac surgery or hepatic artery embolization. As described, a wide range of hemodynamic effects may be encountered perioperatively. These effects can best be avoided or blunted by the preoperative administration of specific hormonal antagonists.
Intravenous octreotide in a dosage of 50 to 100 mg has been shown to reverse intraoperative hypotensive crisis refractory to other therapies. It may be given repeatedly as either a bolus or a continuous infusion. Subcutaneous octreotide is now prescribed both long term and preoperatively for symptom management and to prevent carcinoid crisis. Daily doses to control symptoms range from 50 to 1500 mg given 2 to 4 times a day. Mild hyperglycemia not requiring therapy has been reported, but no major side effects have been noted.
Ketanserin, if available, may be used orally (20 to 40 mg twice daily) for a week before surgery to prevent uncontrollable hypertension or as an intravenous bolus (5 to 10 mg as needed) to treat hypertensive crises perioperatively. It may be given repeatedly. Because of the drug’s potential to cause QT prolongation, hypomagnesemia and hypokalemia should be corrected, and the possible interaction with other drugs that can affect the QT interval should be considered.
Preoperative administration of antihistamines may attenuate the flushing, bronchospasm, and possibly hypotension attributable to histamine, particularly in patients with foregut tumors. The use of diphenhydramine, ranitidine, and cyproheptadine have all been described. These drugs are given the evening before and the morning of surgery. Corticosteroids, which inhibit the synthesis of bradykinins in addition to other actions, are generally given. Intravenous methylprednisolone 1gm given immediately before surgery and intravenous hydrocortisone 100 mg given the evening before and the morning of surgery are both regimens that have been used. Also, the kallikrein inhibitor aprotinin has been used as a perioperative infusion to block the synthesis of bradykinin, it has the added advantage of promoting hemostasis. Case reports have described both low-dose (50.000 to 100.000 KIU) and high-dose (1 million KIU loading dose and 500.00 KIU/ hour) infusions of aprotinin. Data on its efficacy in the carcinoid syndrome are limited and conflicting. Because the high-dose infusions have been shown to decrease the incidence of bleeding after coronary artery bypass grafting surgery, it has been proposed that bleeding may be reduced in carcinoid patients undergoing cardiac surgery as well. The risk of anaphylaxis to aprotinin must be weighed with the risk of catecholamine pressors often needed to manage this reaction.
Although there have been some reports of epinephrine being successfully used in carcinoid patients, it is prudent to avoid the use of catecholamine vasopressors perioperatively. Failure of these drugs to support blood pressure has been reported, and they may exacerbate the hypotension of the carcinoid crisis by stimulating additional production of bradykinin and serotonin. Morphine sulfate has also been shown to stimulate serotonin and histamine release and thus may have adverse hemodynamic consequences. Spinal anesthesia has been reported to precipitate hypotensive crisis. Benzodiazepines and non-histamine-releasing narcotics such as fentanyl have been used safely in carcinoid patients.
Carcinoid tumors are malignant tumors that produce many physiologically active substances. A unique paraneoplastic syndrome consisting of secretory diarrhea, cutaneous flushing, hemodynamic instability, bronchospasm, and structural cardiac disease can result. Although cure rates are low, significant palliation can occur with treatment of the primary tumor as well as of the manifestations of the carcinoid syndrome. Cardiac involvement is common and leads to increased morbidity and early death. Digoxin and diuretics are the cornerstones of medical management for carcinoid heart disease. In the subset of patients with controlled systemic symptoms, good general condition but severe cardiac involvement, and right heart failure, cardiac valve replacement surgery may reduce the short-term mortality rate and alleviate otherwise intractable symptoms. Specific antagonists administered perioperatively and long term may counteract or prevent hemodynamic derangements and debilitating symptoms caused by the tumor’s secretory products.
TABLES
v Table 1. Histologic Types of Carcinoid Tumors
Type A |
Solid nodular nests of cells and peripheral invading cords (Fig 9, Fig 10, Fig 11) |
|
Type B |
Trabecular or ribbon-like structure forming a frequent anastomosing pattern (Fig 12, Fig 13, Fig 14) |
|
Type C |
Tubular-, acinar-, or rosette-appearing structure (Fig 15) |
|
Type D |
Structures with low or atypical differentiation |
|
Mixed Type |
A mixed structure with any combination of the structures above |
v Table 2. Characteristics of Carcinoid Tumors by Site of Origin
|
|
Foregut |
Midgut |
Hindgut |
Location |
Lungs, stomach, duodenum |
Transverse to left colon, rectum |
|
|
Staining |
Argyrophilic |
Argentaffin and argyrophilic |
Neither |
|
Bioactivity: |
|
|
|
5HT |
Low |
High |
None |
|
5HIAA |
High |
High |
Normal |
|
5HTP |
High |
Low |
None |
|
Carcinoid Syndrome |
Occasional |
Frequent |
None |
|
Metastasis |
Bone |
Liver |
Bone |
v Tables 3. Classification and characteristics of carcinoid tumors by site of origin
|
Location (% carcinoids) |
Metastatic potential |
Carcinoid syndrome |
Tumor products |
Symptoms |
|
Foregut |
Moderate to high |
|
|
|
|
Bronchus
|
|
3.5% |
Bronchospasm, atypical flushing, gynecomastia, Cushing syndrome, acromegaly, dilutional hyponatremia, heart disease |
|
|
Stomach |
|
5.0% |
||
|
Proximal duodenum |
|
|
||
|
Midgut |
High |
|
|
|
|
Distal duodenum |
|
80% |
Typical facial flush, hypotension, diarrhea, telangiectasias, wheezing, heart disease |
|
|
Jejunum/ileum (28%) |
|
80% |
||
|
Appendix (45%) |
Low |
|
||
|
Right Colon |
|
|
||
|
Hindgut |
Low |
|
|
|
|
Transverse/ left colon |
|
<1% |
5-HT, tachykinins |
Mild facial flush, diarrhea (both rare) |
|
Rectum |
|
|
MAO, Monoamine oxidase; HCG, human chorionic gonadotropin; ACTH, adrenocorticotropic hormone; 5-HTP, 5-hydroxytryptophan.
v Table 4. Serotonin receptors
|
Receptor type/subtype |
Mechanism |
Binding effect |
|
5-HT1 |
|
|
|
A |
Positive chronotrope and inotrope, smooth muscle vasodilator |
|
|
B |
Inhibits adenylcyclase and norepinephrine release |
Decreases vascular tone |
|
C |
Activates phospholipase C |
Indirect vasodilator; increases EDRF in arterioles |
|
D |
Decreases vascular tone |
|
|
5-HT2 |
Increases phospholipase C and intracellular calcium |
Vasoconstriction mostly in the splanchnic, renal pulmonary, and cerebral beds; hyperglycemia, tachycardia |
|
5-HT3 |
Not elucidated |
Negative chronotrope and inotrope, hypotension and bradycardia by Bezold-Jarisch reflex, depolarizes sensory nerves |
|
5-HT4 |
Adenylcyclase coupled, increases intracellular calcium |
Increases vascular tone |
EDRF, Endothelium – derived relaxing factor.
v Table 5. Demographics and Symptoms of Carcinoid Syndrome
|
|
No Heart Disease |
Heart Disease P |
|||
|
|
n |
% |
n |
% |
|
Race |
|
|
|
|
|
|
White |
487 |
83 |
14 |
74 |
|
|
Other 1 |
97 |
17 |
5 |
26 |
.35 |
Sex |
|
|
|
|
|
|
F |
243 |
42 |
10 |
53 |
.34 |
|
M |
342 |
58 |
9 |
47 |
|
|
Symptoms |
|
|
|
|
|
|
Flushing |
176 |
30 |
16 |
84 |
<.001 |
|
Diarrhea |
259 |
36 |
17 |
89 |
<.001 |
|
Age at Onset of Symptoms, y |
53.1 |
|
53.6 |
|
.89 |
|
Age at diagnosis, y |
54.6 |
|
55.6 |
|
.80 |
1 Given the small numbers in the nonwhite groups, statistical testing necessitated grouping these patients together as “other” for comparison based on the presence or absence of heart disease (Fisher’s exact test). The actual breakdown for “no heart disease” was 91 African Americans, 4 Native Americans, 1 Asian, and 1 Hispanic. The breakdown for “heart disease” was 4 African Americans and 1 Native American.
v Table 6. Number of Patients With Valvular Disease Stratified by Severity
|
|
Mild |
Moderate |
Severe |
Total (%) |
|
Catheterization (out of 13) |
|
|
|
|
|
Tricuspid stenosis |
1 |
4 |
0 |
5 (38) |
|
Tricuspid regurgitation |
… |
0 |
12 |
12 (92) |
|
Pulmonic stenosis |
3 |
1 |
0 |
4 (31) |
|
Pulmonic regurgitation |
2 |
0 |
2 |
4 (31) |
|
Mitral stenosis |
0 |
0 |
0 |
0 (0) |
|
Mitral regurgitation |
4 |
1 |
0 |
5 (38) |
|
Aortic stenosis |
0 |
0 |
0 |
0 (0) |
|
Aortic regurgitation |
0 |
1 |
1 |
2 (15) |
|
Echocardiography (out of 16) |
|
|
|
|
|
Tricuspid stenosis |
4 |
3 |
0 |
7 (44) |
|
Tricuspid regurgitation |
… |
8 |
8 |
16 (100) |
|
Pulmonic stenosis |
4 |
0 |
0 |
4 (25) |
|
Pulmonic regurgitation |
3 |
2 |
1 |
6 (38) |
|
Mitral stenosis |
0 |
0 |
0 |
0 (0) |
|
Mitral regurgitation |
2 |
2 |
0 |
4 (25) |
|
Aortic stenosis |
0 |
0 |
0 |
0 (0) |
|
Aortic regurgitation |
0 |
4 |
0 |
4 (25) |
v Table 7. Hemodynamic Findings in the Subgroup of Cardiac Patients Undergoing Cardiac Catheterization
|
Patient |
RA-V mm Hg |
RA-M mm Hg |
RV-SYS mm Hg |
RVED mm Hg |
PA-SYS mm Hg |
PA-DIA mm Hg |
PA-M mm Hg |
PCW-V mm Hg |
PCW-M mm Hg |
LV-SYS mm Hg |
|
1 |
33 |
24 |
32 |
20 |
32 |
14 |
23 |
22 |
17 |
155 |
|
2 |
25 |
14 |
42 |
10 |
42 |
10 |
20 |
6 |
5 |
150 |
|
3 |
35 |
21 |
46 |
13 |
28 |
12 |
17 |
|
10 |
105 |
|
4 |
30 |
15 |
35 |
16 |
20 |
10 |
14 |
12 |
10 |
122 |
|
5 |
23 |
12 |
25 |
12 |
25 |
7 |
14 |
8 |
11 |
115 |
|
6 |
22 |
12 |
28 |
8 |
25 |
5 |
13 |
7 |
5 |
120 |
|
7 |
20 |
10 |
33 |
8 |
25 |
8 |
14 |
10 |
8 |
120 |
|
8 |
|
25 |
40 |
20 |
30 |
15 |
20 |
|
15 |
125 |
|
9 |
23 |
15 |
32 |
12 |
22 |
9 |
14 |
11 |
10 |
120 |
|
10 |
12 |
8 |
28 |
8 |
28 |
10 |
15 |
14 |
10 |
130 |
|
11 |
22 |
10 |
34 |
10 |
30 |
10 |
14 |
9 |
8 |
190 |
|
12 |
20 |
9 |
24 |
7 |
24 |
8 |
13 |
12 |
8 |
105 |
|
13 |
7 |
4 |
23 |
4 |
20 |
4 |
10 |
7 |
7 |
122 |
|
Mean±SD |
23±8 |
14±6 |
32±7 |
11±5 |
27±6 |
9±3 |
15±4 |
11±5 |
10±4 |
129±23 |
RA-V indicates right atrial v wave; RA-M, right atrial mean; RV-SYS, right ventricular systolic; RVED, right ventricular end-diastolic; PA-SYS, pulmonary artery systolic; PA-DIA, pulmonary artery diastolic; PA-M, pulmonary artery mean; PCW-V, pulmonary capillary wedge v wave; PCW-M, pulmonary capillary mean; LV-SYS, left ventricular systolic; LVED, left ventricular end-diastolic; Ao-SYS, aortic systolic; Ao-DIA, aortic diastolic; Ao-M, aortic mean; CO, cardiac output by the Fick method; CI, cardiac index; and LV-EF, left ventricular ejection fraction.
v Table 8. Survival Estimates by the Product-Limit Method
|
|
|
|
|||
|
|
Survival From Onset of Symptoms, y |
Survival From Time of Diagnosis, y |
|||
|
|
Median |
95% Confidence Interval |
Median |
95% Confidence Interval |
|
|
|
|
|
|
|
|
|
Heart disease |
13.6 |
4.2 – 18.5 |
4.8 |
3.8 – 13.3 |
|
|
|
|
|
|
|
|
|
No Heart disease |
9.7 |
7.3 – 14.0 |
7 |
5.0 – 9.2 |
|
|
|
|
|
|
|
|
v Table 9. Pharmacologic inhibitor therapy in carcinoid disease
|
Medication |
Action |
Indication |
Dosage |
Evidence of efficacy |
|
Octreotide |
Inhibits serotonin release
|
Long-term management |
50-1500 mg SC BID-QID |
CR, series, FDA Approved |
|
Prophylaxis peri-op
Begin at least 24hr in advance of procedure |
50-1500 mg SQ BID-QID or 500 mg IV bolus or 100mg/hr IV infusion |
CR, series |
||
|
|
|
Hypotensive crisis |
50-100 mg IV |
CR, series |
|
Ketanserin |
Blocks serotonin receptors
|
Hypertensive crisis |
5-10mg IV PRN IV drip 5-10mg/hr titrated |
CR, series, Not FDA Approved |
|
Prophylaxis pre-op begin 7 days pre-op |
20-40mg PO BID |
|
||
|
Corticosteroids |
Inhibits bradykinin synthesis Antihistamine effects |
Prophylaxis pre-op |
Methylprednisolone 1gm immediately pre-op or hydrocortisone 100mg IV evening and morning pre-op |
CR, anecdote |
|
Antihistamines |
Blocks histamine receptors |
Symptomatic (bronchospasm, urticaria) |
Standards dosing depending on drug used |
CR, anecdote |
|
H1& H2 blockers Diphenhydramine Ranitidine Cyproheptadine |
|
Prophylaxis pre-op |
25-50mg PO/IV 150mg PO 4mg PO Evening and morning pre-op |
|
|
Aprotinin |
Hemostasis Inhibits Bradykinin synthesis |
After cardiac surgery |
20,000-400,000 KIU IV or 50,000-100,000 KIU/hr IV or 2 million KIU IV + 2 million KIU bypass + 500,000 KIU/hr |
CR CR |
CR, Case report; SC, subcutaneously; IV, intravenously; BID, twice daily; QID, four times daily; FDA food and drug administration; PO, by month
FIGURES
REFERENCES FOR:
MALIGNANT CARCINOID DISEASE
1. Basson MD, Ahlam H, Wangberg B, Modlin IM. Biology and management of the midgut carcinoid. Am J Surg 1993; 165:288-97
2. Mason RA, Steane PA. Carcinoid syndrome: its relevance to the anaesthetist. Anaesthesia 1976; 31:228-42.
3. Garrison JC, Rall TW. Histamine, bradykinin, 5-Hydroxytryptamine and its antagonists. In: Gillman AG, Rall TW, Nies AS, Taylor P, editors. Goodman and Gilman’s the pharmacologic basis for therapeutics. 11th ed. New York: MacMillian, 1994. p. 592-9
4. Conlon JM, Deacon CF, Richter G, Stockmann F, Creutzfeldt W. Circulating tachykinins (substance P, neurokinin A, neuropeptide K) and the carcinoid flush. Scand J Gastroenterol 1987; 22:97-105.
5. Kaplan LM. Endocrine tumors of the gastrointestinal tract and pancreas. In: Isselbacher KJ, Braunwald E, Wilson JD, Martin JB, Fauir AS, Kasper DL, editors. Harrisson’s principles of internal medicine. 13th ed. New York: McGraw Hill, 1994. p. 1538.
6. Kvols LK. Metastatic carcinoid tumors and the malignant carcinoid syndrome. Ann NY Acad Sci 1994; 733:464-70.
7. Ferrans VJ, Roberts WC. The carcinoid endocardial plaque: an ultrastructural study. Hum Pathol 1976; 7:387-409.
8. Pellikka PA, Tajik AJ, Khandheria BK, Seward JB, Callahan JA, Pitot HC, Kvols LK. Carcinoid heart disease. Clinical and echocardiographic spectrum in 74 patients. Circulation 1993; 87:1188-98.
9. Conolly HM, Nishimura RA, Smith HC, Pellikka PA, Mullany CJ, Kvols LK. Outcome of cardiac surgery for carcinoid heart disease. J Am Coll Cardiol 1995; 25:410-6
10. Janson ET, Oberg K. Long-term management of the carcinoid syndrome. Acta Oncologica 1993; 32:225-9.
11. Marsh HM, Martin KJ, Kvols LK, Gracey DR, Warner MA, Warner ME, et al. Carcinoid crisis during anesthesia: successful treatment with a somatostatin analogue. Anesthesiology 1987; 66:89-91
12. Ahlman H, Ahlund L, Dahlstrom A, Martner J, Stenqvist O, Tylen U. SMS 201-995 and provocation tests in preparation of patients with carcinoids for surgery or hepatic arterial embolization. Anesth Analg 1988; 67:1142-8
13. Casthely PA, Jablons M, Griepp RB, Ergin MA, Goodman K. Kestanserin in the preoperative and intraoperative management of a patient with carcinoid tumor undergoing tricuspid valve replacement. Anesth Analg 1986; 65:809-11
14. Houghton K, Carter JA. Peri-operative management of carcinoid syndrome using ketanserin. Anaesthesia 1986; 41:596-9
15. Frishman WH, Huberfeld S, Okin S, Wang Y, Kumar A, Shareef B. Serotonin and serotonin antagonism in cardiovascular and non-cardiovascular disease. J Clin Pharmacol 1995; 35:541-72.
16. Propst JW, Siegel LC, Stover EP. Anesthetic considerations for valve replacement surgery in a patient with carcinoid syndrome. J Cardiothor Vasc Anesth 1994; 8:209-12.
17. Kvols LK, Moertel CG, O’Connell MJ, Schutt AJ, Rubin J, Hahn RG. Treatment of the malignant carcinoid syndrome: evaluation of a long-acting somatostatin analogue. New Engl J Med 1986; 315:663-6.
18. Neustein SM, Cohen E. Anesthesia for aortic and mitral valve replacement in a patient with carcinoid heart disease. Anesthesiology 1995; 82:1067-70.
19. Hamid SK, Harris DNF. Hypotension following valve replacement surgery in carcinoid heart disease. Anaesthesia 1992; 47:490-2.
20. Veall GRQ, Peacock JE, Bax NDS, Reilly CS. Review of the anaesthetic management of 21 patients undergoing lapartomoy for carcinoid syndrome. Br J Anaesth 1994; 72:335-41
21. Camilleri M, Von Der Ohe MR. Drugs affecting serotonin receptors. In: Bailliere’s clinical gastroenterology. London: Bailliere-Tindall, 1994. 301-19.
22. Buchanan KD, Johnston CF, O’Hare MM, et al. Neuroendocrine tumors. A European view. Am J Med. 1986; 81 (suppl 6b): 14-22.
23. Oberg K, Eriksson B. Medical treatment of neuroendocrine gut an dpancreatic tumors. Acta Oncol. 1989; 28 (fasc 3): 425-431
24. Langhans T. Ueber einen drusenpolyp im ileum. Virchow Archiv Pathol Anatom Physio Klin Med. 1867; 38:559-560.
25. Lubarsch O. Uber den primaren krebs des ileum nebst bemerkungen uber das gleichzeitige vorkommen von krebs und tuberculose. Virchow Archiv Pathol Anatom Physiol Klin Med. 1888; 111:280-317
26. Ransom WB. A case of primary carcinoma of the ileum. Lancet. 1890; 2:1020-1023.
27. Oberndorger S. Karzinoide: tumoren des dunndarms. Frnak Z pathol. 1907; 1:426-429
28. Gosset A, Masson P. Tumeurs endocrines de l’appendice. Presse Med. 1914; 2:237-240.
29. Rapport MM, Green AA, Page IH. Partial purification of the vasoconstrictor in beef serum. J Biol Chem. 1948; 174:735-741.
30. Erspamer V, Asero B. Identification of enteramine, the specific hormone of the enterochromaffin cell system, as 5-hydroxytryptamine. Nature 1952; 169:800-801.
31. Lembeck F. 5-Hydroxytryptamine in a carcinoid tumor. Nature. 1953; 172:910-911.
32. Pernow B, Waldenstrom J. Paroxysmal flushing and other symptoms caused by 5-hydroxytryptamine and histamine in patients with malignant tumors. Lancet. 1954; 2:951-953.
33. Page JH, Corcoran AC, Udenfried S, et al. Argentaffinoma as endocrine tumor. Lancet. 1955; 1:198-199.
34. Soga J, Tazawa K. Pathologic analysis of carcinoids: histologic reevaluation of 62 cases. Cancer. 1971; 28:990-998.
35. Johnson LA, Lavin P, Moertel CG, et al. Carcinoids: the association of histologic growth pattern and survival. Cancer. 1983; 51:882-889.
36. Williams ED, Sandler M. The classification of carcinoid tumors. Lancet. 1963; 1:238-239.
37. Moesta KT, Schlag P. Proposal for a new carcinoid tumour stating system based on tumour tissue infiltration and primary metastasis: a prospective multicenter carcinoid tumour evaluation study. West German Surgical Oncologist’s Group. Eur J Surg Oncol. 1990; 16:280-288.
38. Creutzfeldt W, Wtockmann F. Carcinoids and carcinoid syndrome. Am J Med. 1987; 82:4-16.
39. Cheek RC, Wilson H. Carcinoid tumors. Curr Probl Surg. 1970; 7:4-31.
40. Olney JR, Urdaneta LF, Al-Jurf AS, et al. Carcinoid tumors of the gastrointestinal tract. Am Surg. 1985; 51:37-41.
41. Roggo A, Wood WC, Ottinger LW. Carcinoid tumors of the appendix. Ann Surg. 1993; 217:385-390.
42. Chejfec G, Falkmer S, Askensten U, et al. Neuroendocrine tumors of the gastrointestinal tract. Pathold Res Pract. 1988; 183:143-145.
43. Marshall JB, Bodnarchuk G. Carcinoid tumors of the gut: our experience over three decades and review of the literature. J Clin Gastroenterol. 1993; 16:123-129.
44. Warren WH, Gold VE. Neuroendocrine neoplasms of the bronchopulmonary tract: a classification of the spectrum of carcinoid to small cell carcinoma and intervening variants. J Thorac Cardiovasc Surg. 1986; 91:674-689.
45. Gilligan CJ, Lawton GP, Tang LH, et al. Gastric carcinoid tumors: the biology and therapy of an enigmatic and controversial lesion. Am J Gastroenterol. 1995; 90:338-352.
46. Strodel WE, Vinik AI, Thompson NW, et al. Small bowel carcinoid tumors and the carcinoid syndrome. In: Thompson NW, Vinik AI, eds. Endocrine Surgery Update. New York, NY: Grune and Stratton; 1983: 227-291.
47. Moertel CL, Weiland LH, Telander RL. Carcinoid tumor of the appendix in the first two decades of life. J Pediatr Surg. 1990; 25:1073-1075.
48. Akerstrom G, Makridis C, Johansson H. Abdominal surgery in patients with midgut carcinoid tumors. Acta Oncol. 1991; 30:547-553.
49. Basson MD, Ahlman H, Wnagberg B, et al. Biology and management of the midgut carcinoid. Am J Surg. 1993; 165:228-297.
50. Orloff MJ. Carcinoid tumors of the rectum. Cancer. 1971; 28:175-180.
51. McCaughan BC, Martini N, Bains MS. Bronchial carcinoids: review of 124 cases. J Thorac Cardiovasc Surg. 1984; 89:8-17.
52. Norheim I, Oberg K, Theodorsson-Norheim E, et al. Malignant carcinoid tumors: an analysis of 103 patients with regard to tumor localization, hormone production, and survival. Ann Surg. 1987; 206:115-125.
53. Eriksson B, Oberg K. Peptide hormones as tumor markers in neuroendocrine gastrointestinal tumors. Acta Oncol. 1991; 30:477-483.
54. Rea F, Binda R, Spreafico G, et al. Bronchial carcinoids: a review of 60 patients. Ann Thorac Surg. 1989; 47:412-414.
55. Rozenman J, Pausner R, Lieberman Y, et al. Bronchial adenoma. Chest. 1987; 92:145-147.
56. Lowe JE, Bridgman AH, Sabiston DC Jr. The role of bronchoplastic procedures in the surgical management of benign and malignant pulmonary lesions. J Thorac Cardiovasc Surg. 1982; 83:227-234.
57. Bordi C, Yu JY, Baggi MT, et al. Gastric carcinoids and their precursor lesions: a histologic and immunohistochemical study of 23 cases. Cancer. 1991; 67:663-672.
58. Sjoblom SM, Haapiainen R, Miettinen M, et al. Gtastric carcinoid tumours and atrophic gastritits. Acta Chir Scand. 1987; 153:37-43.
59. Eckhauser FE, Lloyd RV, Thompson NW, et al. Antrectomy for multicentric, argyrophil gastric carcinoids: a preliminary report. Surgery. 1988; 153:37-43.
60. Richards AT, Hinder RA, Harrison AC. Gastric carcinoid tumour associated with hypergastrinaemia and pernicious anaemia-regression of tumors by antrectomy: a case report. S. Afr Med J. 1987; 72:51-53.
61. Davies MG, O’Dowd G, McEntee GP, et al. Primary gastric carcinoids: a view on management. Br J Surg. 1990; 77:1013-1014.
62. Deans GT, Spence RA. Neoplastic lesions of the appendix. Br J Surg. 1995; 82: 299-306.
63. Thompson GB, van Heerden JA, Martin JK Jr, et al. Carcinoid tumors of the gastrointestinal tract: presentation, management, and prognosis. Surgery. 1985; 98:1054-1063.
64. Godwin JD. Carcinoid tumors: an analysis of 2837 cases. Cancer. 1975; 36:560-569.
65. Rindi G, Luinetti O, Cornaggia M, et al. Three subtypes of gastric argyrophil carcinoid and the gastric neuroendocrine carcinoma; clinicopathologic study. Gastroenterology. 1993; 104:994-1006.
66. Vinik AI, Strodel WE, Llyod R, et al. Unusual gastroenteropancreatic tumors and their hormones. In: Thompson NW, Vinik AI, eds. Endocrine Surgery Update. New York, NY: Grune and Stratton; 1983:293-300.
67. Vinik AI, Thompson N, Ecklauser F, et al. Clinical features of carcinoid syndrome and the use of somatostatin analogue in its management. Acta Oncol. 1989; 28 (fasc 3): 389-402.
68. Ahlman H, Dahlstrom A, Gronstad K, et al. The pentagastrin test in the diagnosis of the carcinoid syndrome: blockade of gastrointestinal symptoms by ketanserin. Ann Surg. 1985; 201:81-86
69. Norheim I, Theodorsson-Norheim E, Brodein E, et al. Tachykinins in carcinoid tumors: thei ruse as a tumor marker and possible role in the carcinoid flush. J Clin Endocrinol Metab. 1986; 63:605-612.
70. Norton JA, Sugarbaker PH, Doppmon JL, et al. Aggressive resection of metastatic disease in selected patients with malignant gastrinoma. Ann. Surg. 1986; 203:352-359.
71. Martin JK Jr. Moertel CG, Adson MA, et al. Surgical treatment of functioning metastatic carcinoid tumors. Arch Surg. 1983; 118:537-542.
72. McEntee GP, Nagorney DM, Kvols LK, et al. Cytoreductive hepatic surgery for neuroendocrine tumors. Surgery. 1990; 108:1091-1096.
73. Carrasco CH, Charnsangavej C, Ajani J, et al. The carcinoid syndrome: palliation by hepatic artery embolization. AJR Am J Roentgenol. 1986; 147:149-154.
74. Cho KJ, Reuter SR, Schmidt R. Effects of experimental hepatic artery embolization on hepatic function. AJR Am J Roentgenol. 1976; 127:563-567.
75. Coupe MO, Hodgson HJF, Hemingway A, et al. The effect of hepatic artery embolization on survival in the carcinoid syndrome. J Intervent Radiol. 1989; 4:179-181.
76. Makowka L, Tzakis AG, Mazzaferro V, et al. Transplantation of the liver for metastatic endocrine tumors of the intestine and pancreas. Surg Gynecol Obstet. 1989; 168:107-111.
77. Arnold JC, O’Grady JG, Bird GL, et al. Liver transplantation for primary and secondary hepatic apudomas. Br J Surg. 1989; 76:248-249.
78. Kvols LK, Metastatic carcinoid tumors and the carcinoid syndrome: a selective review of chemotherapy and hormonal therapy. Am J Med. 1986; 81:49-55.
79. Kvols LK, Moertel CG, O’Connell MJ, et al. Treatment of the malignant carcinoid syndrome: evaluation of a long-acting somatostatin analogue. N Engl J Med. 1986: 315:663-666.
80. Wangberg B, Nilsson O, Theodorsson E, et al. The effect of a somatostatin analogue on the release of hormones from human midgut carcinoid tumour cells. Br J Cancer. 1991; 64:23-28.
81. Harris AG, O’Dorisio TM, Woltering EA, et al. Consensus statement: octreotide dose titration in secretory diarrhea. Dig Dis Sci. 1995; 40:1464-1473.
82. Diaco DS, Hajarizadeh H, Mueller CR, et al. Treatment of metastatic carcinoid tumors using multimodality therapy of octreotide acetate, intra-arterial chemotherapy, and hepatic arterial chemoembolization. Am J Surg. 1995; 169:523-528.
Carcinoid tumors are endocrinologic malignancies often associated with a characteristic syndrome – the malignant carcinoid syndrome.
Cardiovascular manifestations of this rare illness result from unique pathophysiologic characteristics, are associated with poor prognosis, and are difficult to treat medically. The hemodynamic consequences of this disease present unique management problems perioperatively. New pharmacologic and surgical therapies for malignant carcinoids have improved quality of life for patients to extent that carcinoid heart disease now has more impact on morbidity and mortality rates. Cardiologists may be called on to diagnose and treat this rare cardiac disease. We review, for consulting cardiologists, the pathophysiologic characteristics, cardiovascular manifestations, and management of this disease.
Année: 2001
Auteurs: Alfred F.AMMOURY
Gino S. GEMAYEL
Wissam F. DERIAN
Titre de Thèse: Complications Cardiovasculaires des Tumeurs Carcinoïdes Malignes.
Résumé: Les tumeurs carcinoïdes sont les tumeurs endocriniennes les plus rencontrées au niveau du tractus digestif. Elles se trouvent surtout au niveau de l’appendice. Elles secrètent des substances bioactives différentes (Surtout la sérotonine) qui sont responsables du syndrome carcinoïde (Diarrhée, Flushing, Bronchoconstriction, Hypotension). Les manifestations cardiovasculaires résultent de caractéristiques pathophysiologiques (Via récepteur 5-HT 2B), sont associées à un mauvais pronostic et sont difficiles à traiter médicalement. Le traitement primaire des tumeurs carcinoïdes est chirurgical, ceux qui sont non resécables ou bien largement métastatiques peuvent subir une chirurgie de cytoréduction et/ou une embolization de l’artère hépatique qui sera suivie par une palliation des symptômes par l’octréotide qui est un analogue de la somatostatine. L’atteinte cardiaque (Régurgitation tricuspidienne et pulmonaire) peut être traitée par un remplacement valvulaire.
Mots clés: Tumeurs carcinoïdes, Métastase hépatique, Sérotonine, 5-HT 2B, Bradykinines, Syndrome carcinoïde, Diarrhée, Flushing, Bronchoconstriction, Hypotension, Insuffisance cardiaque droite, Plaque, Régurgitation tricuspidienne, Régurgitation pulmonaire, Résection chirurgicale, Chirurgie de cytoréduction, Embolization de l’artère hépatique, Octréotide, Somatostatine, Remplacement valvulaire
Summary: Carcinoid tumors are the most frequently encountered endocrine tumors of the GI tract. They are most often found in the appendix. They may secrete a variety of bioactive substances (Especially serotonin), which are associated with the carcinoid syndrome (Diarrhea, Flushing, Bronchoconstriction, Hypotension). Cardiovascular manifestations result from unique pathophysiologic characteristics (Via 5-HT 2B receptor), are associated with poor prognosis, and are difficult to treat medically. The primary treatment for a carcinoid tumor located anywhere in the gut is surgical. Those who have widely metastatic disease or who are anatomically unresectable may undergo cytoreductive surgical debulking and/or hepatic arterial embolization followed by palliation of symptoms with octreotide, the long-acting somatostatin analog. Cardiac involvement (Tricuspid and pulmonary regurgitation) may be treated by valvular replacement.
Keywords: Carcinoid tumors, Hepatic metastases, Serotonin, 5-HT 2B, Bradykinins, Carcinoid syndrome, Diarrhea, Flushing, Bronchoconstriction, Hypotension, Right side heart failure, Cardiac plaque, Tricuspid regurgitation, Pulmonary regurgitation, Surgical resection, Cytoreductive surgery, Hepatic arterial embolization, Octreotide, Somatostatin, Cardiac valve replacement.
Directeur de Thèse: Dr. Hadi KARAA
![]()
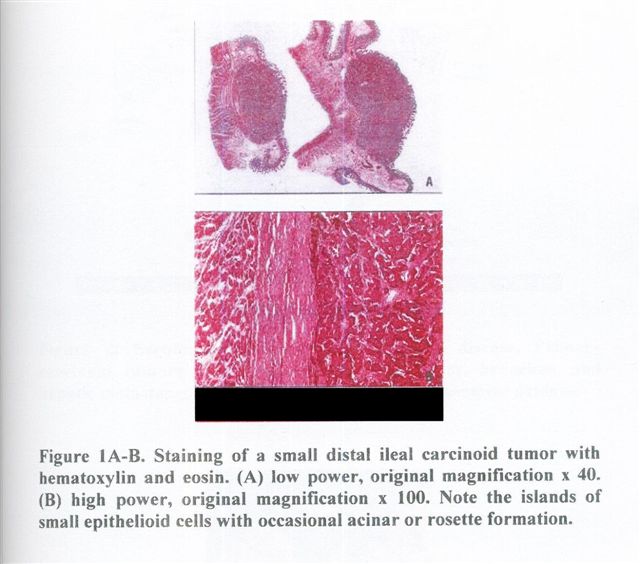{kind=link}
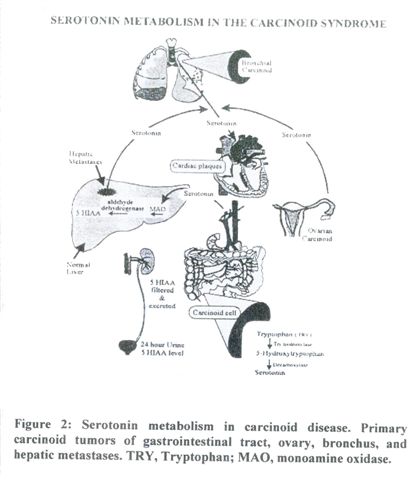{kind=link}
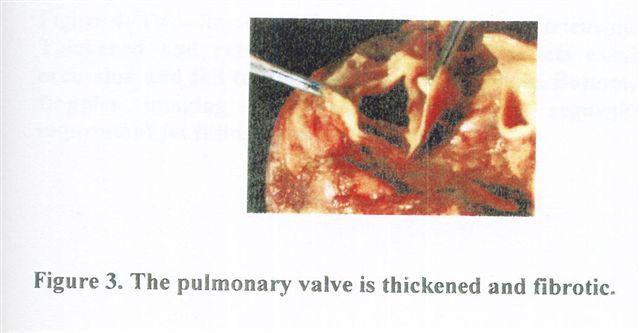{kind=link}
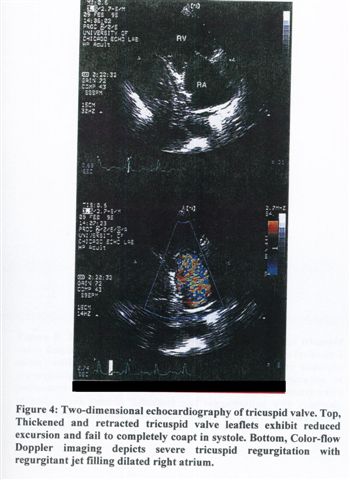{kind=link}
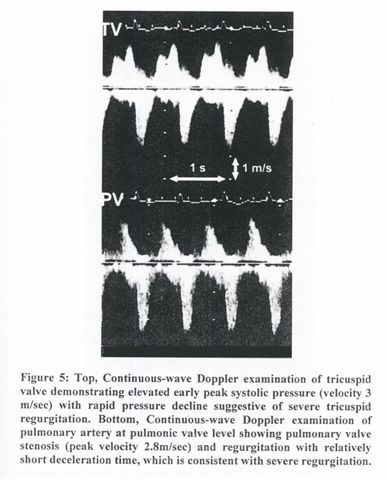{kind=link}
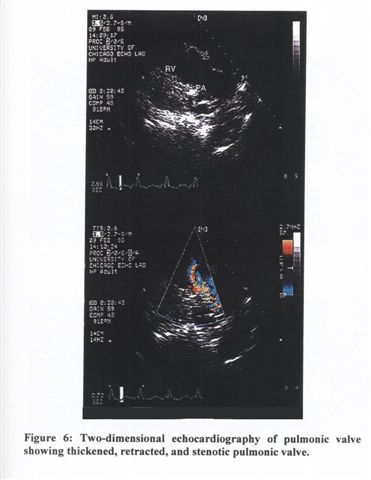{kind=link}
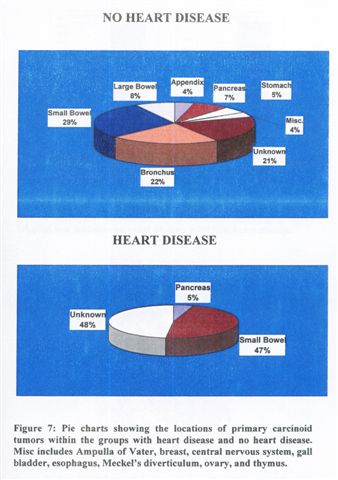{kind=link}
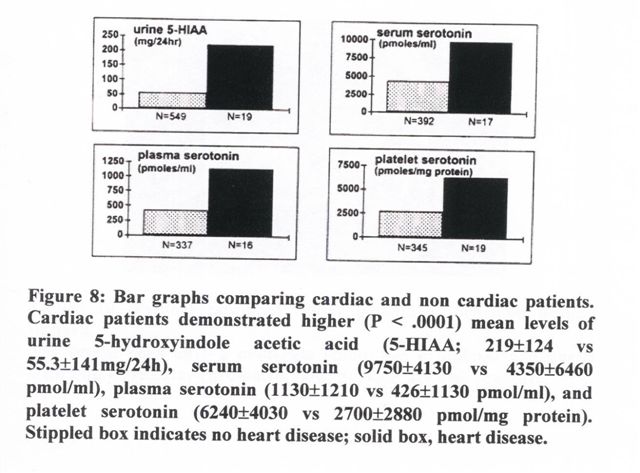{kind=link}
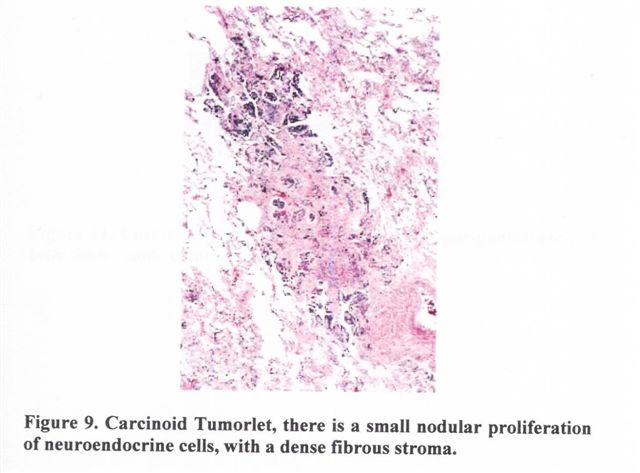{kind=link}
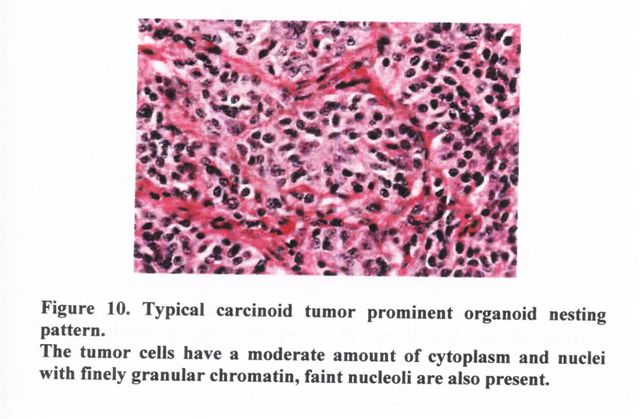{kind=link}
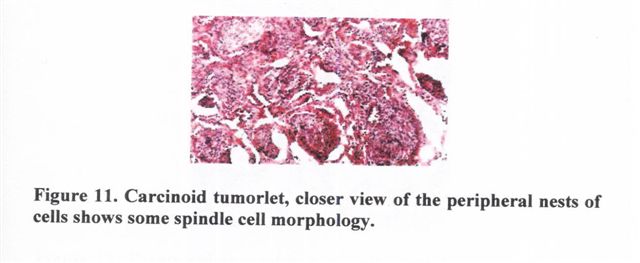{kind=link}
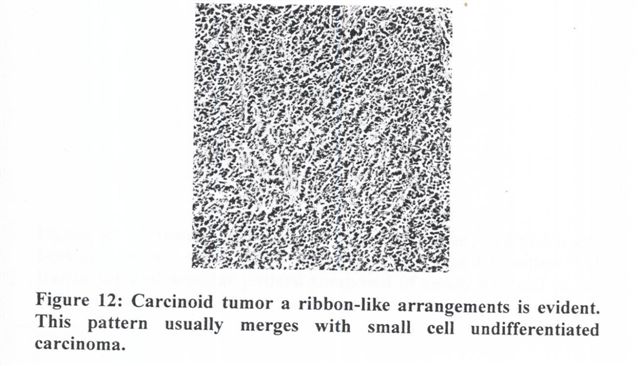{kind=link}
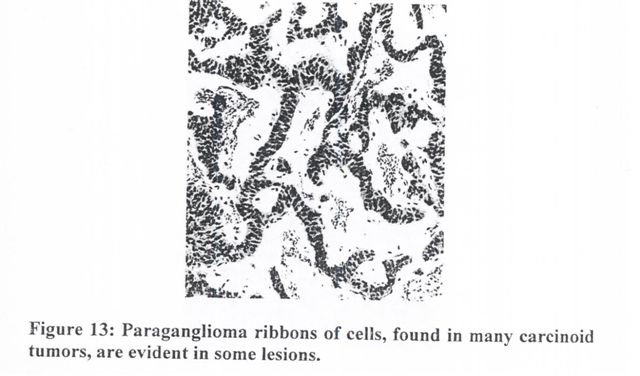{kind=link}
{kind=link}
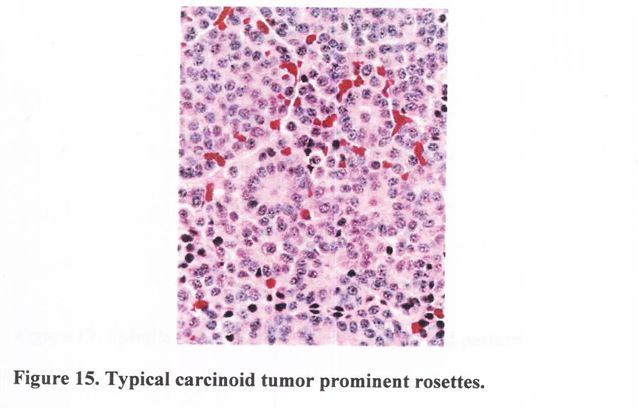{kind=link}
{kind=link}
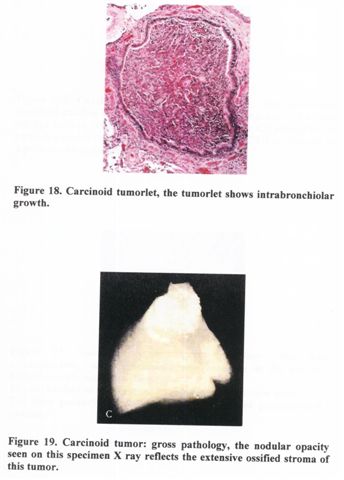{kind=link}
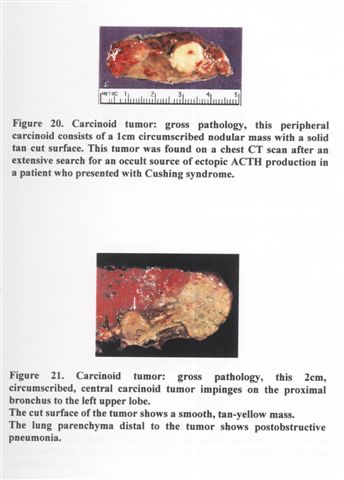{kind=link}
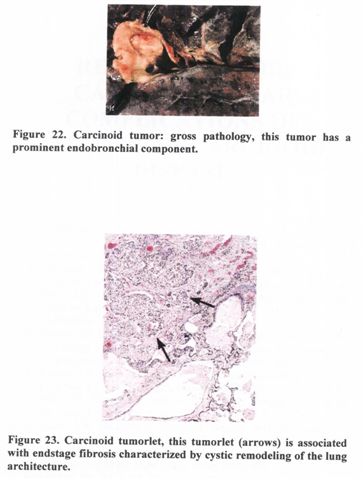{kind=link}